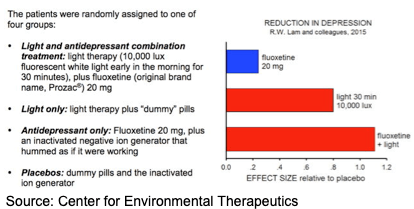
Fortunately, Canadian psychiatrist Raymond Lam has now put antidepressants to the acid test. In a study in the November 2015 Journal of the American Medical Association, Dr. Lam and his colleagues pitted antidepressants against light therapy — not for SAD, but for the far more common major depression that can occur at any time of year.
What do you need to know to make light therapy work for you?
 Get the right light box. The Center for Environmental Therapeutics (CET), the go-to source of wisdom on light, mood, energy, and sleep, defines the criteria to look for.
Get the right light box. The Center for Environmental Therapeutics (CET), the go-to source of wisdom on light, mood, energy, and sleep, defines the criteria to look for.- The right time for sessions depends on the individual. Find out the best time for you to initiate light therapy with a free self-assessment, the automated Morningness-Eveningness Questionnaire (AutoMEQ).
- Tweak light therapy as needed. For example, some people need more than 30 minutes per day. Others want to combine light therapy with supplementary treatment (including antidepressants that have had only partial effect). A professional, a friend who successfully uses light therapy, or even some recommended reading and free fact sheets may give you useful information, or an understanding of what makes light therapy work.
And if you have questions, you can submit them to CET’s Ask the Doctor, a free service. Just first Search the questions that have already been answered.
Most important, especially if you have been taking an antidepressant, is to discuss these new findings with your doctor, and decide together whether and how you should bring light therapy into your daily life.